Fluid Responsiveness vs. Fluid Tolerance
Stop Drowning the “Responsive” Patient

The “Sepsis Bundle” Reflex
It’s 2 AM in the ICU again. A septic patient rolls in hypotensive. The resident performs a Passive Leg Raise (PLR), sees a 15% bump in Stroke Volume (or VTI), and declares victory: “They are fluid responsive! Let’s bolus another liter!”
Two liters later, the MAP is barely holding at 65 mmHg, but the FiO2 has climbed to 60%, crackles are echoing through the lungs, and we are scrambling for the intubation kit.
What happened? We mistook responsiveness for a green light, ignoring the body’s plea for mercy (Responsive + Non-Tolerant). Responsiveness is merely a description of the heart’s mechanical state; it is not a prescription for volume.
The Lesson: Just because the heart can pump more fluid, doesn’t mean the rest of the body should receive it. Chasing the Frank-Starling curve blindly often leads to drowning the patient.
Part 1: The Physiology of “Responsiveness” (Forward Flow)
“Will more preload boost cardiac output?” This is Fluid Responsiveness in a nutshell. It answers a purely mechanical question about the Left Ventricle’s position on the Frank-Starling curve.
A ΔSV > 10-15% with a fluid challenge or PLR. Most healthy people are fluid responsive. If I gave you a liter of saline right now, your Stroke Volume would go up. Does that mean you need a liter of saline? No. Responsiveness is often a physiologic normality, not a pathologic deficiency. Treating a “responsive” patient who has a replete tank is how we create iatrogenic salt water drowning.
Case: The “Responsive” Athlete. Imagine a young athlete in the ED after a marathon. They are “responsive” to a PLR. But their IVC is fully collapsing and their organs are perfusing. We don’t bolus them because they are responsive; we rehydrate them because they are volume depleted.
Part 2: The Physiology of “Tolerance” (The Venous Congestion)
We must look at the Venous Side. Fluid Tolerance asks: “What is the metabolic cost of this fluid on the right heart and downstream organs?” The veins aren’t bottomless pits. Boosting Mean Systemic Filling Pressure can spike Central Venous Pressure, choking organ drainage.
Organ perfusion pressure = MAP - CVP. When CVP rises, perfusion pressure drops. The result is Congestive Nephropathy (venous-backup AKI) and gut edema (which worsens sepsis via bacterial translocation).
Case: The Congested Kidney. Mr. Patel, 55, post-op with an anastomotic leak. He is PLR responsive. However, his baseline CVP is 12 mmHg and his creatinine is rising. If we bolus him, we might bump his MAP, but we will crush his GFR by raising his renal vein pressure. Tolerance flags what responsiveness misses.
Part 3: The Solution - VExUS and the “Stop Sign”
The VExUS score was originally introduced by Beaubien-Souligny et al. in post-cardiac surgery patients, where portal flow pulsatility and severe intrarenal venous flow alterations were independently associated with AKI, improving prediction beyond CVP alone. Longino et al. (2023) prospectively validated VExUS against right heart catheterization, demonstrating a strong correlation with right atrial pressure (R² = 0.68) and an AUC of 0.99 for predicting RAP ≥ 12 mmHg, far superior to IVC diameter alone (AUC 0.79). So, how do we know when the tank is full? CVP alone is notoriously unreliable.
Enter the VExUS Score (Venous Excess Ultrasound Grading System). Think of this as your hemodynamic “Stop Sign.” It looks at the transmission of pressure waves backwards from the Right Atrium into the abdominal organs.
“How-To”:
Probe: Phased Array (Cardiac) or Curvilinear (Abdominal).
Vital: You must have an EKG tracing on your screen. You cannot interpret systolic (S) vs. diastolic (D) flow without knowing when the heart is squeezing.
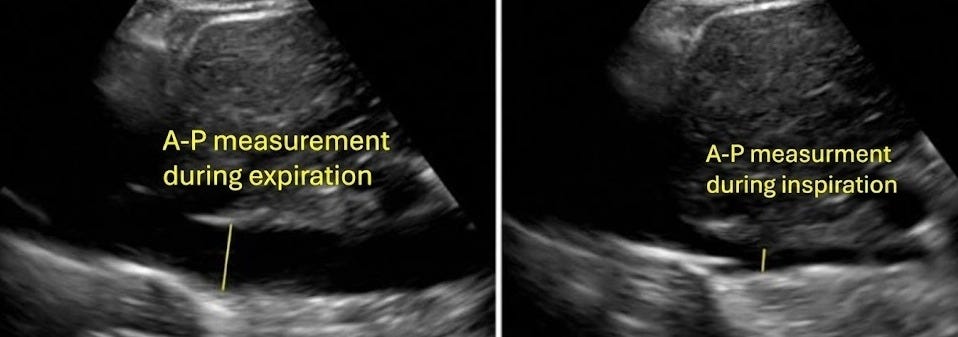
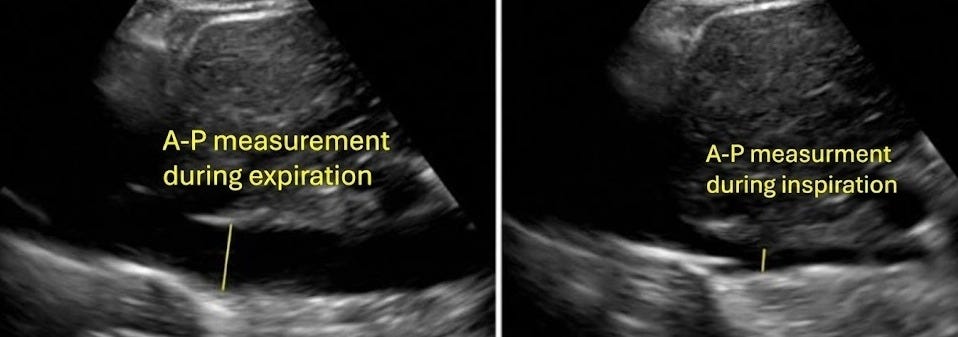
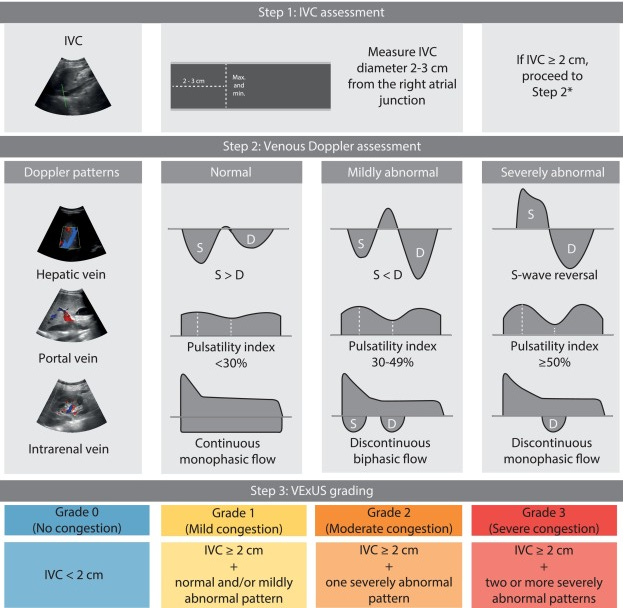
1. The Gateway: Inferior Vena Cava (IVC) Start at the subxiphoid.
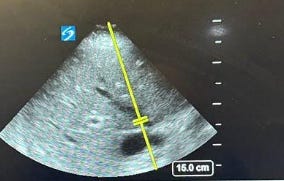
The Check: If the IVC is small (<2cm) and collapsing, stop. You have fluid tolerance.
The Red Flag: If it is plethoric (>2 cm) and non-collapsing, the door is open for pressure transmission. You must proceed to the organs.
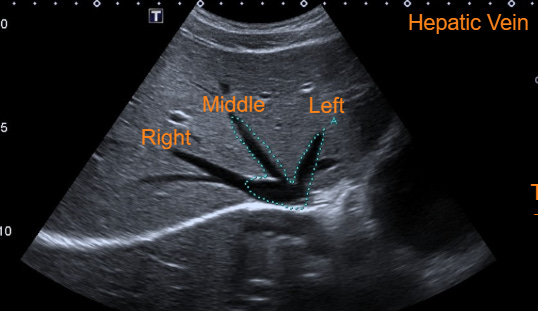
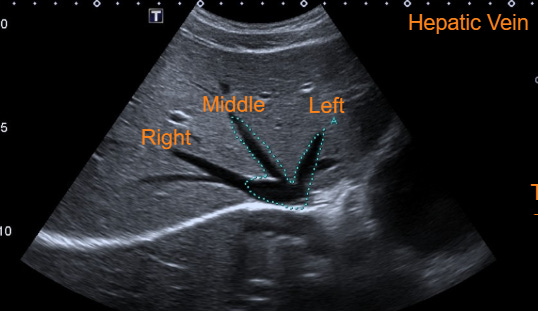
2. Hepatic Vein (The First Stop) Still in subxiphoid, slide slightly to the patient’s right and angle up. Find the “bunny ears” draining into the IVC.
The Technique: Put your Pulsed Wave (PW) Doppler gate about 1-2 cm inside the vein.
Normal: S-wave is larger than D-wave.
Abnormal: The S-wave gets smaller. In severe congestion, it reverses (S-Reversal)
3. Portal Vein (The Early Warning) Move to the Right Upper Quadrant (mid-axillary line), just like a FAST exam. Find the main Portal Vein entering the liver hilum (thick, echogenic walls).
The Technique: Flow is usually “red” (towards the probe).
Normal: Continuous, monophasic flow. Like a gentle hum.
Abnormal: It starts to wave. If you see Pulsatility Fraction > 50%, the liver is sensing high pressure. This is often the first sign of trouble.

4. Intra-Renal Vein: Go to the posterior axillary line (kidney view). Turn on Color Doppler to find the interlobar vessels (the tiny ones in the cortex, not the main renal vein).
The Technique: Zoom in. Drop your PW gate over a specific interlobar grouping.
Normal: Continuous flow below the baseline (venous) with arterial spikes above.
Abnormal: “Diastolic Interruptions.” The flow stops or reverses during diastole because the pressure inside the kidney is too high for blood to exit.

Important Nuances
A critical perspective from Guinot (2025) emphasizes that VExUS reflects complex interactions between cardiac function, filling pressures, and volume status rather than pure volume assessment, patients with the highest VExUS scores often have cardiogenic shock despite low fluid balance, while those with significant volume excess may have low scores when cardiac function is preserved. Guinot et al. (2022) found that the portal pulsatility index was the best predictor of appropriate response to diuretic-induced fluid depletion (AUC 0.80), outperforming the composite VExUS score (AUC 0.66).
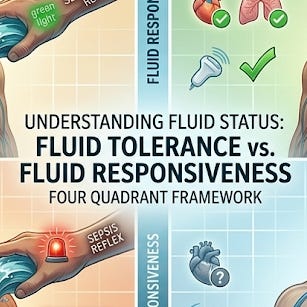
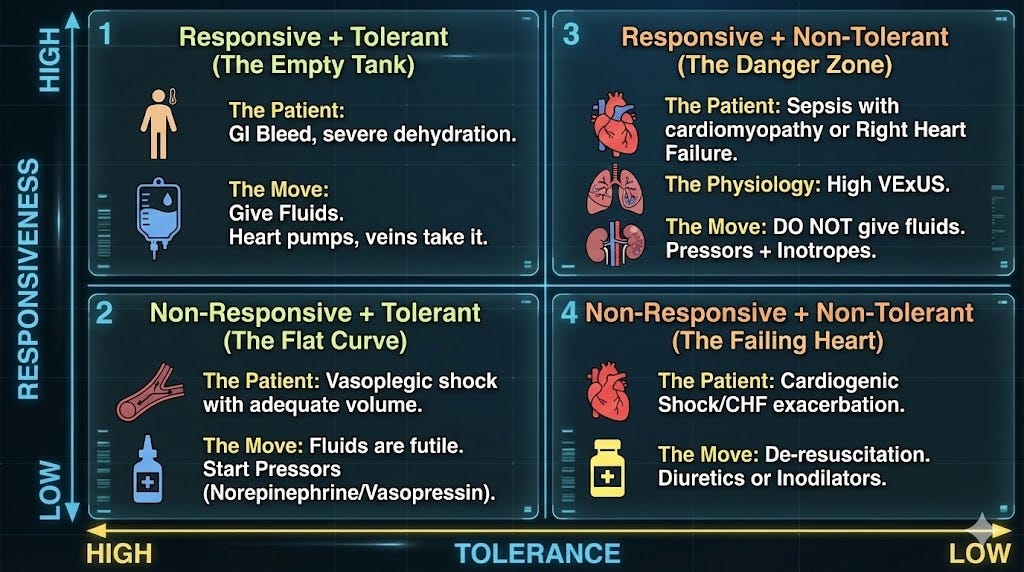
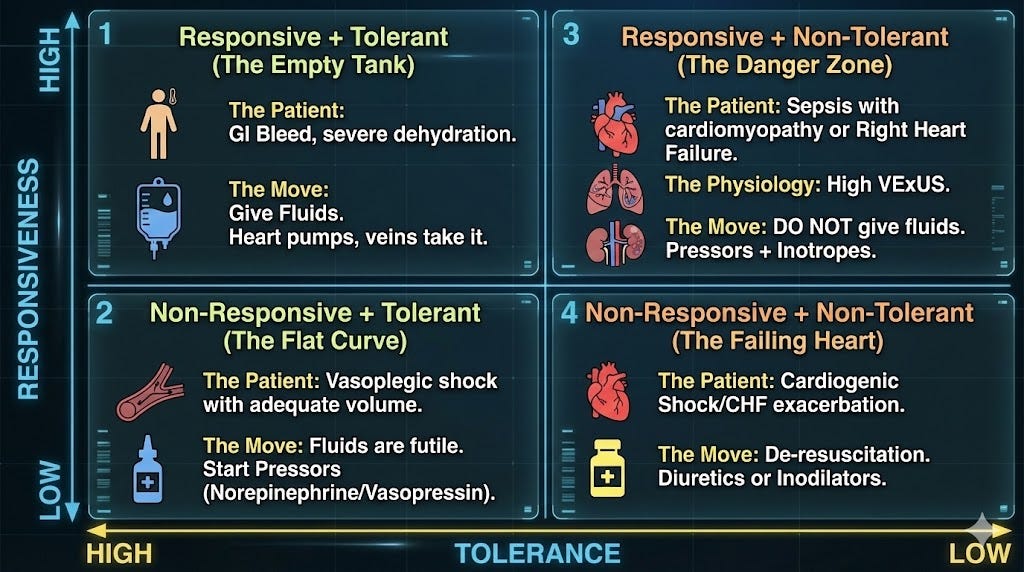
The Clinical Algorithm: The 4 Quadrants
When evaluating the hypotensive patient, I don’t just ask “Are they responsive?” I map them onto a Responsiveness vs. Tolerance matrix.
Quadrant 1: Responsive + Tolerant (The Empty Tank)
Patient: GI Bleed, severe dehydration.
Give Fluids. The heart can pump it, and the veins can take it.
Quadrant 2: Non-Responsive + Tolerant
Patient: Vaso-plegic shock with adequate volume.
Fluids are futile. Start Pressors (Norepinephrine/Vasopressin).
Quadrant 3: Responsive + Non-Tolerant
Patient: Sepsis with cardiomyopathy or Right Heart Failure. The LV could pump more, but the RV/Lungs/Kidneys are already full (High VExUS).
Do NOT give fluids. Use pressors to tighten the tank rather than filling it. You need inotropes, not volume.
Quadrant 4: Non-Responsive + Non-Tolerant (The Failing Heart)
Patient: Cardiogenic Shock/CHF exacerbation.
De-resuscitation. Diuretics or Inodilators.
“Hemodynamically stable” is not just a MAP > 65 mmHg, it is a balance between adequate flow and absence of congestion. Stop treating “Fluid Responsiveness” as a command. Treat it as permission.
Responsiveness tells you if you can give fluid.
Tolerance (VExUS/Lungs) tells you if you should.
In the ICU, the amateur chases the MAP; the master protects the endothelium.
Thanks for reading.
Asim
Educational Disclaimer: All ultrasound images, Doppler waveform tracings, and diagrams used in this post are reproduced solely for non-commercial educational purposes under fair use. Images have been sourced from the following references and their original authors retain all rights. This content is for educational purposes only and is intended for medical professionals. It does not constitute medical advice. Clinical guidelines and protocols vary by institution; always follow your local hospital protocols and use clinical judgment when treating patients.
References:
Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock 2026.
Fluid Therapy for Critically Ill Adults With Sepsis: A Review.3.
Fluid Response Evaluation in Sepsis Hypotension and Shock: A Randomized Clinical Trial.
Cardio-Pulmonary-Renal Interactions: A Multidisciplinary Approach.
Prospective Evaluation of Venous Excess Ultrasound for Estimation of Venous Congestion.
VExUS Score: Optimizing Its Use in Perioperative and Critical Care Management.
A Comprehensive Review of Venous Excess Ultrasound (VExUS) Score: Evidence From Original Research.
The Use of Venous Doppler to Predict Adverse Kidney Events in a General ICU Cohort.